Week of November 27, 2023
With time off for Thanksgiving, my older son at home, and driving with my younger son (to accumulate the Maryland learner's permit required hours), I've received abundant teenage feedback regarding my verbal idiosyncrasies and most common discussion themes. I am confident (as in I have been repeatedly reminded, sometimes in group settings) that my children will remember me for pithy sayings like, "everybody has an agenda," and frequently describing opportunities and choices in terms of "trade-offs." I suspect they are not wrong - at least when measured by how many times I write about tensions, trade-offs, and debate in today's newsletter. However, my kids and I differ in our interpretation of their comments. I see young adults rebelling to differentiate and discover a mature identity. My older son claims he is offering "free introspective therapy guiding me on the road to middle-age self-improvement." It's all relative, I suppose.
---
U.S. hospitalization rates are down 3% over the last 14 days. Wastewater COVID RNA concentrations are rising. I anticipate increasing cases following Thanksgiving, but with a lack of uniform testing or case reporting, it may take a few weeks to see changes based on hospitalizations alone.
The NY Times COVID Tracker reflects only CDC-gathered hospital data. Hospitalization data are a (lagging) indicator.
https://www.nytimes.com/interactive/2023/us/covid-cases.html
Wastewater monitoring is more of a LEADING indicator.
The Inside Medicine COVID dashboard
------
COVID articles
The most provocative articles and threads I've seen this week are about the high volume of sick individuals in China, South Korea, and France - primarily children with high fever, cough, and chest X-ray findings of nodules. The illness is described as "walking pneumonia" and seems most consistent with mycoplasma, a tiny bacteria spread via respiratory droplet. (To be clear, there is also probably RSV and flu.). These events are provocative due to the association between this new outbreak and the reports of COVID-induced immune suppression. That is, mycoplasma pneumonia is not uncommon. However, some armchair (and real) scientists hypothesize that some individuals who had COVID have "injured" immune systems and are more susceptible. Others discuss a scientifically unproven notion of "immunity debt." Irrespective of why, the rapid rise in pneumonia cases is stoking fear of "yet another pandemic." While we await more data, the debate amongst healthcare professionals is educational: What are we dealing with? What is the relationship to COVID? At what point do we re-institute masking and other pandemic policies? (By the way, N95 masks, air filtration, and isolation are protective against airborne or droplet-transmissible organisms.)
Best consumer article I have seen:
Some commentary worth reading:
Public Health student Sabina Vohra-Miller and Infectious disease Dr. Samira Jeimy on the fallacy of immunity debt and the more real notion of immune system damage:
https://twitter.com/sabivm/status/1588658173866823682
and
Dr. Ashish Jha on why he is not worried:
https://twitter.com/ashishkjha/status/1728198816007098569
and
Dr. Jeremy Faust on the data we know to date:
https://insidemedicine.substack.com/p/pneumonia-clusters-among-children
Sometimes, journal articles demonstrate early data that you hope stand up to more rigorous investigation. A Taiwanese group of researchers found an association between coffee consumption and decreased risk of COVID in population databases. They did further benchtop research demonstrating that coffee (freshly ground or instant, regular or decaf, with or without sugar, cream, or milk) inhibited coronavirus entry into cells in a test tube. And while early (and a bit bold), the authors conclude, "This study verified moderate coffee consumption, including decaffeination, can [assist in preventing] SARS-CoV-2. [W]e also suggest a coffee-drinking plan [to] prevent infection in the post-COVID-19 era." I will eagerly prescribe coffee-drinking plans (at least for myself). Starbucks, as best I can tell, did not fund this research.
and
https://cellandbioscience.biomedcentral.com/articles/10.1186/s13578-023-01154-9
Medical Trends and Technology
Dr. Eric Topol shared a fantastic infographic on the long physiology, genetics, and drug development journey that led to the approval of GLP-1 drugs (like Ozempic). The graphic is a reminder of why bringing a compound to market typically takes decades and billions of dollars.
https://twitter.com/erictopol/status/1727408513151008812
The graphic is from a firewalled Science article: https://www.science.org/doi/10.1126/scitranslmed.adh4453
Note the 1st comment in the Twitter thread - "Do you think A.I. will accelerate this?" Answer: "Yes."
Last week, social media captured a heartbreaking story that exemplifies many frustrations of the U.S. healthcare system. The events are about a young mother with a genetically linked form of rapidly advancing lung cancer whose insurance company initially agreed to pay for a lung transplant. However, the insurance company reneged at the last minute - while the patient was at the hospital for the surgery. A lot is happening in the story - physicians trying to find good outcomes (in the face of low-probability of success), the limits of what we can and cannot detect (such as when small numbers of cancer cells spread), medical technology's ethical and clinical boundaries, social media outrage, and healthcare paid for by large, private insurers. I do not often agree with Dr. Vinay Prasad, but he did a good job describing the nuance and complexities of these events in his blog. While this scenario is atypical, analogs of these events will be more common. I suspect the coming wave of CRISPR-based care will increase the need to ask who receives and pays for expensive and (perhaps) unproven therapies.
https://www.sensible-med.com/p/should-insurance-companies-pay-for
Dr. Richard Byyny is an internist and the executive director of the national medical honor society Alpha Omega Alpha (AOA) (like Phi Beta Kappa for doctors). In the fall AOA newsletter editorial, he argues, "[It is time for a] national doctor-patient care time study, or series of studies, to document the best length for a doctor's visit to provide the best caring and quality of care[...]." His idea is laudable - the "standard 15-minute appointment" is far too short for managing even typical illness - often the intersection of genetics, socioeconomics, and behavior. Moreover, the growth of complex diagnostic and therapeutic options feels exponential. Ironically, I suspect any such study will result in an answer he doesn't like - more A.I. and technology, bolstering the workforce with less expensive non-physician clinicians (like nurses and advanced practitioners), and more standardization of care (like algorithms or protocols). His editorial is an excellent example of the tension between optimizing revenue, the finite nature of time, and healthcare's endless potential for demand generation.
https://www.alphaomegaalpha.org/wp-content/uploads/2023/11/pp3-8-Editorial_AUT23.pdf
Infographics
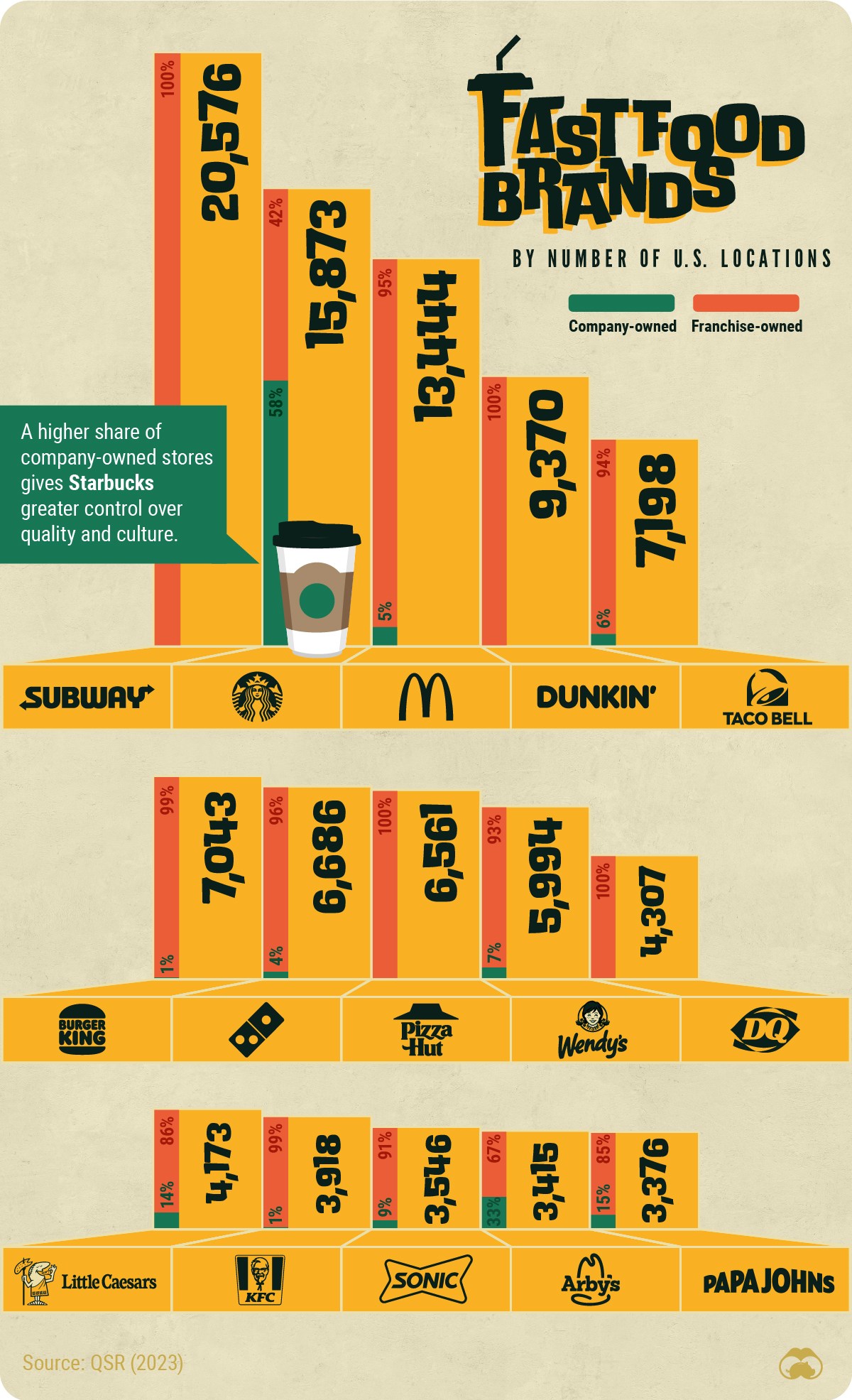
U.S. Fast Food brands ranked by number of locations. The accompanying article is even more interesting. Subway has 20,500 locations. That is amazing.
https://www.visualcapitalist.com/wp-content/uploads/2023/11/Fast-Food-Brands-by-Location.jpg
{kind=link}
from
https://www.visualcapitalist.com/fast-food-brands-with-the-most-u-s-locations/
Things I learned this week
A quiet breakfast on a holiday weekend staring at a box of oatmeal spawns the question, "What makes Irish oats Irish?"
https://www.tastingtable.com/947939/irish-vs-scottish-oats-whats-the-difference/
Moments later I was down the rabbit hole - reading about the breakout winners from the World Porridge Championship - a yearly competition in which contestants deftly and artfully manipulate cut oats, water, salt, heat, and time - all aiming to take home The Golden Spurtle.
https://www.bbc.com/news/uk-scotland-highlands-islands-67053001
and
https://www.instagram.com/forridge_uk/
All of this begs the next obvious question - WTF is a spurtle? I learned spurtles are the Swiss Army Knife of Scottish kitchen utensils.
https://en.wikipedia.org/wiki/Spurtle
and
https://www.epicurious.com/expert-advice/what-is-spurtle-how-to-cook-with-it-article
But wait! It is far more complex! Spurtles come in Scottish and German subtypes, with an origin (perhaps) from the Roman Army:
https://wildcherryspoonco.com/products/spurtle-flat-couthie-solid
During informal polling on spurtle knowledge in my household, my son hypothesized that "spurtle" may be the most "double entendreable" word ever. I suggest you ask ChatGPT for "a list of words most often used in double entendre" and judge for yourself.
Living with A.I.
Last week's drama surrounding Sam Altman (the fired, re-hired CEO from OpenAI) highlights a series of discussions I've seen in recent weeks about the balance between rapid innovation and ethics/safety. It is not just A.I., but the rapidity of LLM development drives the conversation.
The Guardian offered a thoughtful article on the politics of OpenAI's "accelerationists" and "decelerationists."
Here is a related Twitter thread on the trade-offs of Space X's rapid-cycle innovation (in other words, failing fast in the aerospace industry may not be like failing fast elsewhere).
https://twitter.com/tazerface16/status/1726258692071583851?s=42&t=cHtDhpWgAdi0UhIayqsoag
And, in sticking with the theme of trade-offs of failing fast, Elon Musk and A.I. - Neuralink obtained FDA approval for clinical trials in humans, despite recent concerns about their primate testing program.
and
https://www.wired.com/story/elon-musk-nerualink-congress-sec-letter/
A.I. art of the week
"An overly-complex schematic of a steampunk porridge-making pot with an integrated spurtle."
https://drive.google.com/file/d/1us6SwLja5qFagqXb-isgTUi5dZPTsuXk/view?usp=sharing
DALL-E made a drawing that is the visual equivalent of the famous Turbo Encabulator video from the 1980s:
https://youtu.be/2fjcJp_Nwvk?si=X7e0Mm2jNsnn4Wwt
Clean hands and sharp minds, team,
Adam
Comments
Post a Comment